

Dealing with My Cancer Diagnosis


“You have cancer.”
More than 1.6 million Americans hear those words every year, according to the Centers for Disease Control and Prevention.
Learning that I had cancer last August came as a shock because I had no symptoms and still don’t.
That doesn’t make the cancer any less threatening, so I’m finally going to have major surgery tomorrow.
My type of cancer (I still haven’t completely wrapped my head around calling it “my” cancer) was considered extremely rare, but a sharply increasing number of Americans are getting diagnosed with it.
I’ve chosen to share my experience because the journey has involved many ups and downs, and I’ve learned a series of lessons that I hope will be useful.
When Did I Get Sick?
I didn’t get sick, at least not when it came to any specific illness caused by the cancer.
I did begin to have weird stomach pains in early 2021. For most people, that’s probably not terribly unusual. But I often joke that growing up in Latin America made me develop a stomach of steel. I dismissed the pains as stress, because I disliked my job and was working way too hard under intense deadlines.
The pains were also sporadic, so I stupidly did not emphasize them to my longtime doctor, Ramon Leon, during my yearly physical in the spring.
Lesson No. 1: Tell your doctor if anything unusual is going on, even if you don’t think it’s a big deal.
The stomach pains became more consistent in the summer, so I went back to see Dr. Leon in early August. He figured out I had an umbilical hernia, but was concerned enough about the other symptoms that he told me to call a gastroenterologist and get both a colonoscopy (I wasn’t due to get one for another five years) and an upper endoscopy (more specifically an esophagogastroduodenoscopy or EGD), a procedure that involves inserting a long, flexible tube through your mouth and esophagus to visually examine the upper part of your digestive system.
I texted a friend and well-known gastroenterologist, Dr. Eduardo Ruan, and he said I should go see him. He agreed with Dr. Leon, and we scheduled the colonoscopy/EGD for September.
In the few weeks in between, I changed jobs, immediately decreasing my stress levels. My stomach pains, except those clearly connected to the hernia, disappeared. I considered canceling everything.
Thank God I didn’t.
Initial Diagnosis
While Dr. Ruan didn’t see anything of major concern and thought everything looked good during the endoscopy, he biopsied a few small polyps. A week later, he got the results and called me with the bad news.
If you are going to be told you have cancer, you want to get the news from someone like Dr. Ruan. He gently explained that one of the biopsies had found a relatively rare and slow-growing neuroendocrine tumor (NET) in my duodenal bulb.
I confess, I had no idea what any of that meant.
Making matters worse, the terminology surrounding NETs is very confusing. They are also referred to as “carcinoid tumors,” and, in a series of my medical reports from various medical centers, “benign” carcinoid tumors. You can see one example in the picture below.

This image shows part of a medical report following an enteroscopy I had on May 18, 2022. It refers to a tumor as a "benign carcinoid tumor."
First, there’s nothing benign about them, as an article from the MD Anderson Cancer Center says: “Now, all neuroendocrine tumors are considered malignant. There are just shades of gray in terms of how aggressive they are.”
Second, “carcinoid” doesn’t mean a tumor is precancerous or just similar to cancer. Carcinoid tumors, according to the Mayo Clinic, are a type of slow-growing cancer that can arise in several places throughout your body, most commonly in the digestive tract. The carcinoid tumors/NETs often don’t cause signs or symptoms until late in the disease, usually not before they’ve started to metastasize and become a much more serious problem.
The bottom line is that I had cancer, but my tumor was small (a mass of less than half an inch), with well-differentiated cells that indicated the cancer was grade 1 and slow-growing. As Dr. Ruan emphasized, I could very well die of something else before the NET became a problem.
That did not mean I could sit around to wait and see.
How Did I React?
I am different than most people in that I never go through the five stages of grief.
My conscious mind jumps immediately to acceptance, focuses on the questions to ask and the actions to undertake, and doesn’t fall into denial, anger, bargaining, or depression. I tend not to dwell on worst-case scenarios, other than to make sure my affairs are in order so that if things go far worse than expected, no matter how unlikely, my family isn’t further burdened.
The cancer, for my conscious mind, is simply another challenge to overcome.
I wish I could say the same for my subconscious mind, which does see monsters come out at night. In my nightmares, the cancerous cells, slow-growing and unthreatening as they may be, metastasize and spread fatally. Sleep turns to anxiety, almost always at around 4 a.m. Kindle and Xanax then become essential companions.
Fortunately, the nightmares have been infrequent, and they haven’t distracted from the challenge.
What Then?
Lesson No. 2: Don’t hesitate, don’t wait. Everything is going to take longer than you think.
The immediate need was to figure out how to get rid of the tumor. A regular endoscopy couldn’t do it, so the next step was to get an endoscopic ultrasound with a specialist, Dr. Daniel Gelrud. I was lucky that an appointment opened within a month, in early November.
Not so lucky is that the procedure resulted in a double whammy: It confirmed the tumor was too difficult to access for resection by even the fancier endoscopy, and Dr. Gelrud found a second tumor in the duodenal bulb.
It was time to see a surgical oncologist who specializes in this kind of cancer.
Dr. Ramon Jimenez, the chief of the Division of Melanoma and Soft Tissue Sarcomas at the Miami Cancer Institute gave me an appointment quickly.
The news wasn’t great. Even though the tumors were small, their placement required major surgery and a rewiring of my digestive tract. Specifically, I needed a gastrojejunostomy with a partial duodenectomy.
In layman’s terms, the surgery involves cutting off the duodenal bulb (the top of the duodenum, where the stomach empties into the small intestine), closing off that exit from the stomach, and then connecting the stomach directly to the jejunum (the middle part of the small intestine). That would allow food and other stomach contents to flow from the stomach straight to the jejunum, bypassing the duodenum.
The image below shows the small intestine, and the one below that is a rough drawing, derived from one made by Dr. Jimenez, that illustrates the procedure. My apologies for my terrible drawing and handwriting.
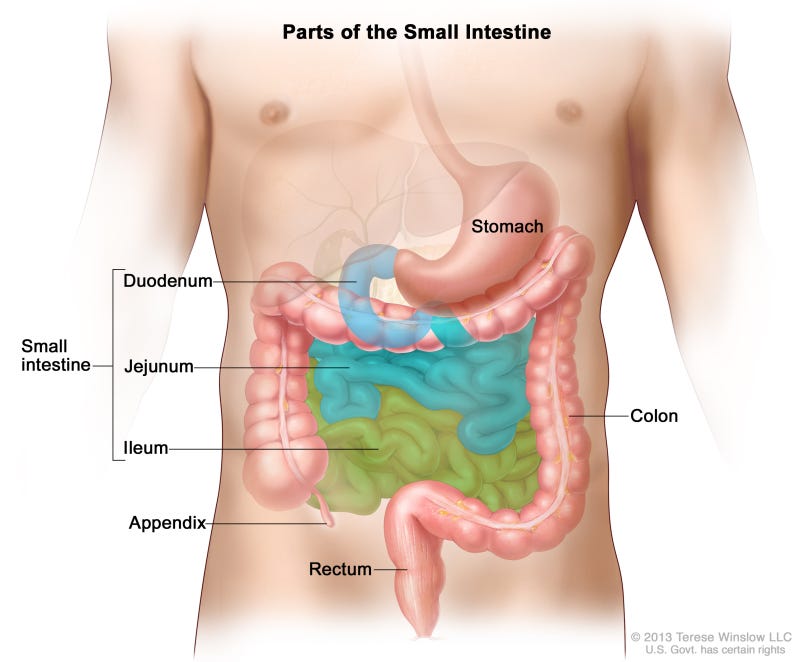
Courtesy: National Institutes of Health
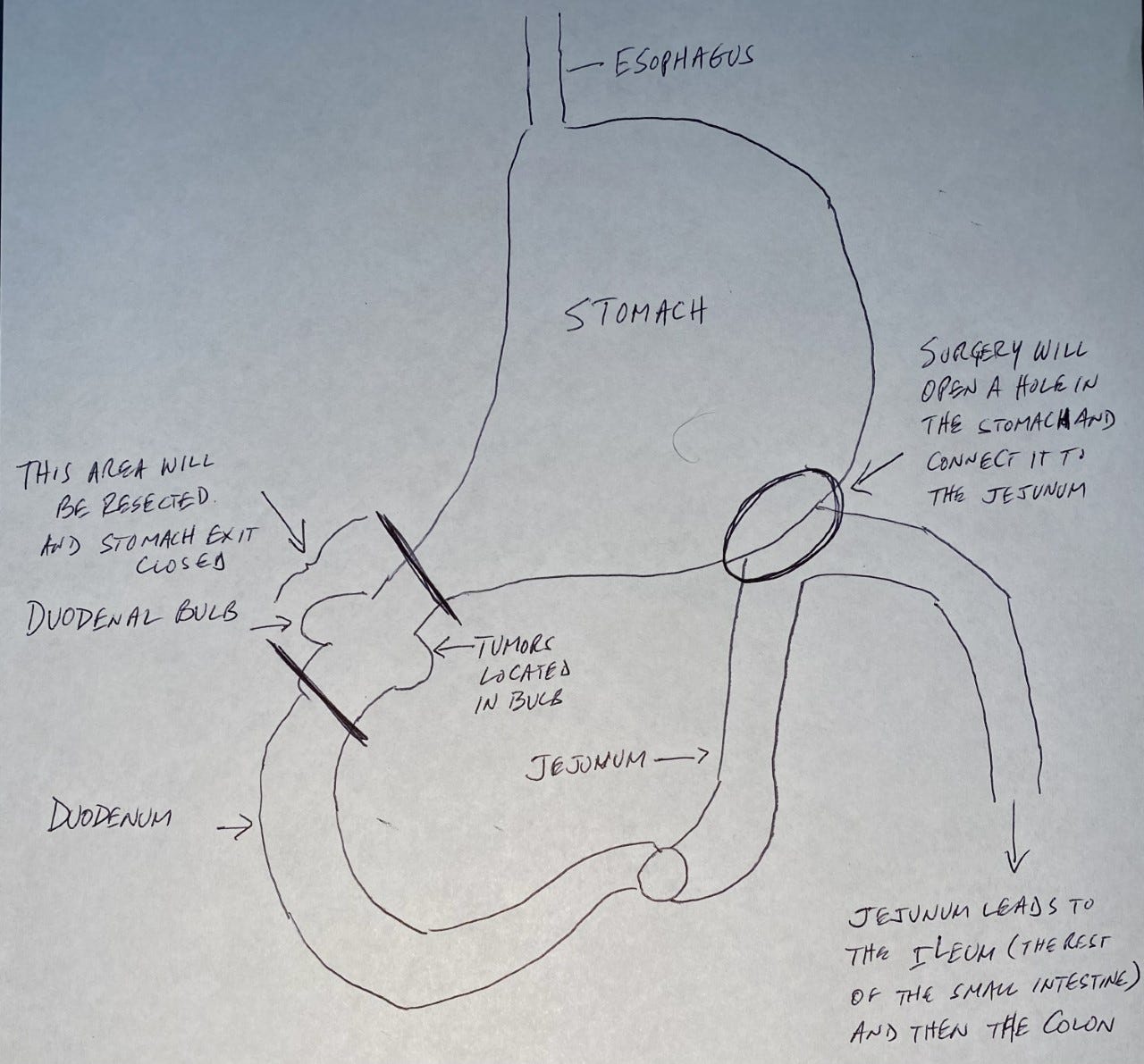
My terrible drawing of what the surgery will entail.
What Had to Happen Before Surgery?
First, I needed all sorts of testing. In December, a CT scan of the abdomen and pelvis and a chest X-ray found nothing else of concern (in fact, the CT scan didn’t even see the tumors).
To make sure I was fit for surgery, I then had a cardiac workup like nothing I’d heard of before. The nurses said the stress test results showed I was as fit as a guy in his 30s. I suspect they say that to everyone.
I also had a capsule endoscopy to make sure no other tumors existed. This procedure involves swallowing a tiny camera that’s contained in a capsule that’s bigger than any pill you’ve ever seen. If that’s not bad enough, the combination of the prep for it and the restrictions on eating for many hours after taking the capsule were almost as bad as what’s involved in a colonoscopy.
The camera takes pictures as it works its way through the digestive tract. You then expel it through a bowel movement, retrieve it (fun), and send it to a lab that reads the results.
While we waited to learn what those were, friends and family pushed me to get a second opinion and consider traveling to have my surgery at New York’s Memorial Sloan Kettering Cancer Center.
A lifelong friend, Dr. Sergio Giralt, one of the world’s authorities on blood disorders, works there. He connected me to Dr. Makoto Nishimura, one of the top experts on using endoscopies to remove growths, and Dr. Vivian Strong, a renowned surgeon who specializes in the kind of procedure proposed by the doctors here in Miami. The Sloan Kettering physicians concurred completely with the Miami doctors. Still, I considered going to New York to have the surgery, which is what my family wanted, but the rapid spread of Omicron in December and January eliminated any desire we had to travel there.
Lesson No. 3: Get a second opinion. Even if it just validates the first opinion, it will give you peace of mind.
At this point, in early January, I received the results of the capsule endoscopy. They threw another wrench into the works, indicating I might have a third tumor, in the jejunum.
I suddenly needed even more tests to figure out what is going on, so surgery in January was now off, postponed to March.
The main test was a PET scan with a recently developed radioactive tracer called Gallium GA 68-Dotatate that binds to NETs, clearly showing them anywhere in the body on the PET scan images.
When I went in for the scan in mid-February, I even talked to the technician about what was being done to make sure it was the correct procedure. Unfortunately, a miscommunication occurred with the radiology imaging center, so I was injected with a different dye. The good news is that it found that I had no other cancer or cardiovascular issues between the base of my skull and my thighs. The bad news is that the PET scan they did does not detect all NETs.
So, I had to go back to the drawing board, and postpone the surgery again.
I finally had the proper PET scan in mid-March, and it did not find a tumor in the jejunum, but confirmed “positive tumor activity” in the duodenal bulb. That was followed by an enteroscopy (an endoscopy that goes further down into the small intestine) in mid-May that further confirmed there was no third tumor.
Lesson No. 4: You can’t get enough information about your procedures in order to make sure you’re getting what’s needed.
Should People Screen for NETs?
A study published in the Journal of Global Oncology in 2016 points out that “NETs are uncommon” and that “The journey of the patient with a NET has rarely been documented.” That’s despite the fact that “Incidence rates continue to increase, partly because of greater awareness of the disease and increased accuracy of diagnosis.” In fact, the study found that the incidence of NETs has increased five-fold over the past 30 years.
Still, the number of cases remains fairly low. The Cleveland Clinic says only about 12,000 cases are diagnosed each year in the U.S.
Another old friend, Dr. David Loeb, the former director of endoscopy at the Mayo Clinic in Jacksonville who remains an emeritus consultant there, explained that “Most NETs that are not part of a syndrome are diagnosed incidentally, meaning a person would have an endoscopy or radiographic imaging study for another reason and these, usually small lesions, are found.”
So should people get regular endoscopies, like mammograms, colonoscopies, or prostate cancer screenings?
Dr. Jimenez’s answer is emphatically no, pointing out the relatively low incidence of NETs, the cost of the endoscopies, and the danger of false positives. He points out that early-detection tests make sense for high-incidence diseases like breast cancer (more than a quarter million cases diagnosed annually in the U.S.), colorectal cancer (more than 150,000 cases per year), or prostate cancer (almost 270,000 yearly cases).
As Dr. Loeb put it, “Because NETs are relatively rare and more indolent (slow-growing) than other gastrointestinal cancers, we do not currently recommend screening the entire population for these tumors. But, as diagnostic tests, including hormonal, genetic, and immunologic techniques improve and increase in number, there is reason to believe these tumors will be detected more frequently and likely at even earlier stages.”
Conclusion
I hope that wasn’t too much information and that it is useful to at least some of you. While I made every attempt to be accurate, I am not a physician, so I urge you to please talk to your doctor if you are concerned about anything in this article.
It’s odd to have major surgery even though I couldn’t feel any better and have no related symptoms.
But I certainly did not want to live knowing that I have malignant cells growing inside, no matter how slow-growing they might be, and all doctors I spoke to concurred with my decision.
I will post you on how things go. Wish me luck and keep me in your prayers.
Cover photo: A picture of me with my dog, Albus, because I couldn't think of anything better to post.
Please let me know what you think by leaving a comment below. You can also do so on my Facebook page (https://www.facebook.com/antoniomoraTV1/). Please subscribe (it's free) and share the link: https://aviewfromthecenter.bulletin.com/subscribe.